
Incidence and mortality of lung cancer in China, 2008−2012
Introduction
Among global males, lung cancer is the most common cancer of incidence and a leading cause of death from cancer. Among females, lung cancer is the third most common cancer of incidence and the second most common cause of death from cancer. According to GLOBOCAN 2018, there was about 2.1 million new cases and 1.8 million deaths worldwide in 2018 (1). Lung cancer is also a common cancer site and a major cause of death from cancer and causes a greater disease burden in China. Previous papers have reported the national incidence and mortality rates based on data from a specific year (2-4). In order to eliminate the influence of annual random change of rates and guarantee the stability of statistical results, we describe the epidemic characteristics of lung cancer in China to provide basic information for the control and research of lung cancer, using a 5-year consolidated database pooled from 2008 to 2012.
Materials and methods
Cancer registry data source
National Central Cancer Registry (NCCR) of China collected cancer registration data from population-based cancer registries in China. A total of 164 cancer registries in China submitted the registration data from 2008 to 2012 and the data of 135 cancer registries were included in pooled data for analysis according to the criteria of quality control. Among the 135 cancer registries there were 56 registries located in urban areas and 79 registries located in rural areas. These cancer registries covered a population of 629,333,910 person-years (318,623,600 males and 310,710,310 females, 382,669,450 urban areas and 246,664,460 rural areas). The analysis data of lung cancer (International Statistical Classification of Diseases and Related Health Problems 10th Revision, ICD-10 C33 and C34) including incidence, death records and annual population are derived from the database of NCCR. Furthermore, each year, rate of incidence/mortality of lung cancer and the data of population during 2003−2007 were acquired from the database of NCCR.
Quality control
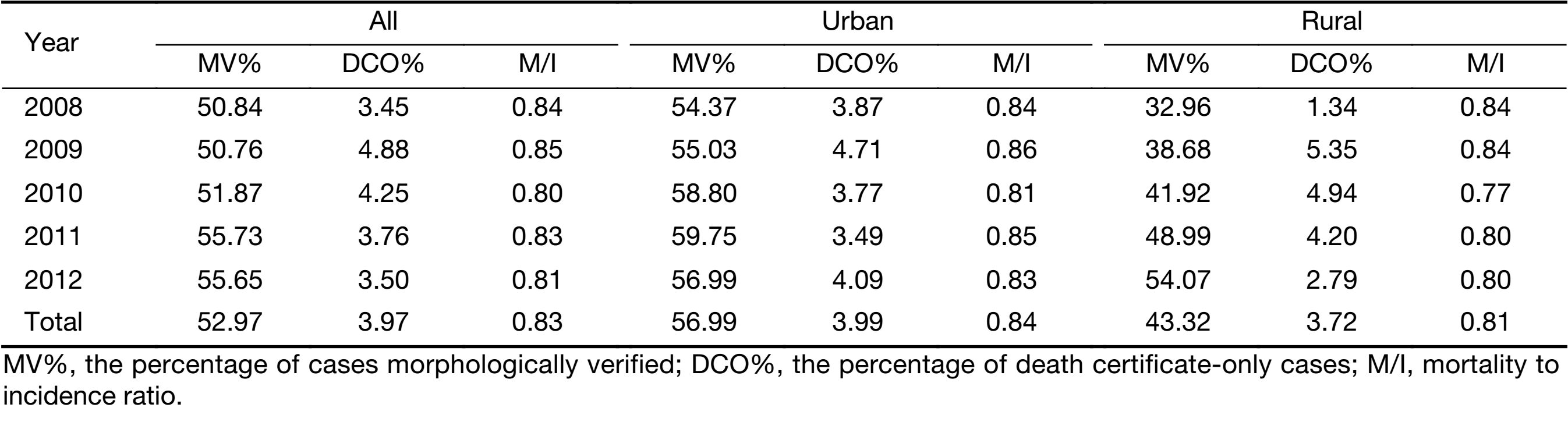
Cancer registry data submitted to NCCR underwent quality control based on the criteria of “Guideline for Chinese Cancer Registration” (5) and “Cancer Incidence in Five Continents Volume IX” by International Agency for Research on Cancer/International Association of Cancer Registries (IARC/IACR) (6). The validity, reliability, completeness and comparability of cancer registry data were evaluated based on a comprehensive consideration of a series of indexes including the mortality to incidence (M/I) ratio, the percentage of cases morphologically verified (MV%), and the percentage of death certificate only cases (DCO%) (4). In the present analytical data of lung cancer, MV% was accounted for 52.97%, DCO% was 3.97% and the ratio of M/I was 0.83. In urban cancer registries, those indictors were 56.99%, 3.99% and 0.84, respectively. In rural cancer registries, the MV%, DCO% and the ratio of M/I were 43.32%, 3.72% and 0.81, respectively (Table 1).
Full table
Statistical analysis
Cancer registration areas were classified into urban or rural areas according to the National Bureau of Statistics of the People’s Republic of China. Crude cancer incidence and mortality rates of lung cancer were calculated by area (urban/rural), region (eastern, middle, western), gender (male, female) and age groups (0−, 1−4, 5−84 by 5 years and 85+years). The Chinese standard population in 2000 and Segi’s world population were applied to determine age-standardized incidence and mortality rates. The cumulative risk of developing or dying from cancer before 75 years old was calculated and presented as a percentage. The annual percentage change (APC) of the rate was calculated for time trend analysis from 2003 to 2012. SAS software (Version 9.4; SAS Institute Inc., Cary, NC, USA) and Joinpoint Regression Program (Version 4.5.0.1; Statistical Methodology and Applications Branch, Surveillance Research Program, National Cancer Institute, Rockville, MD, USA) were used for statistical analysis. P<0.05 was considered statistically significant.
Results
Incidence of lung cancer
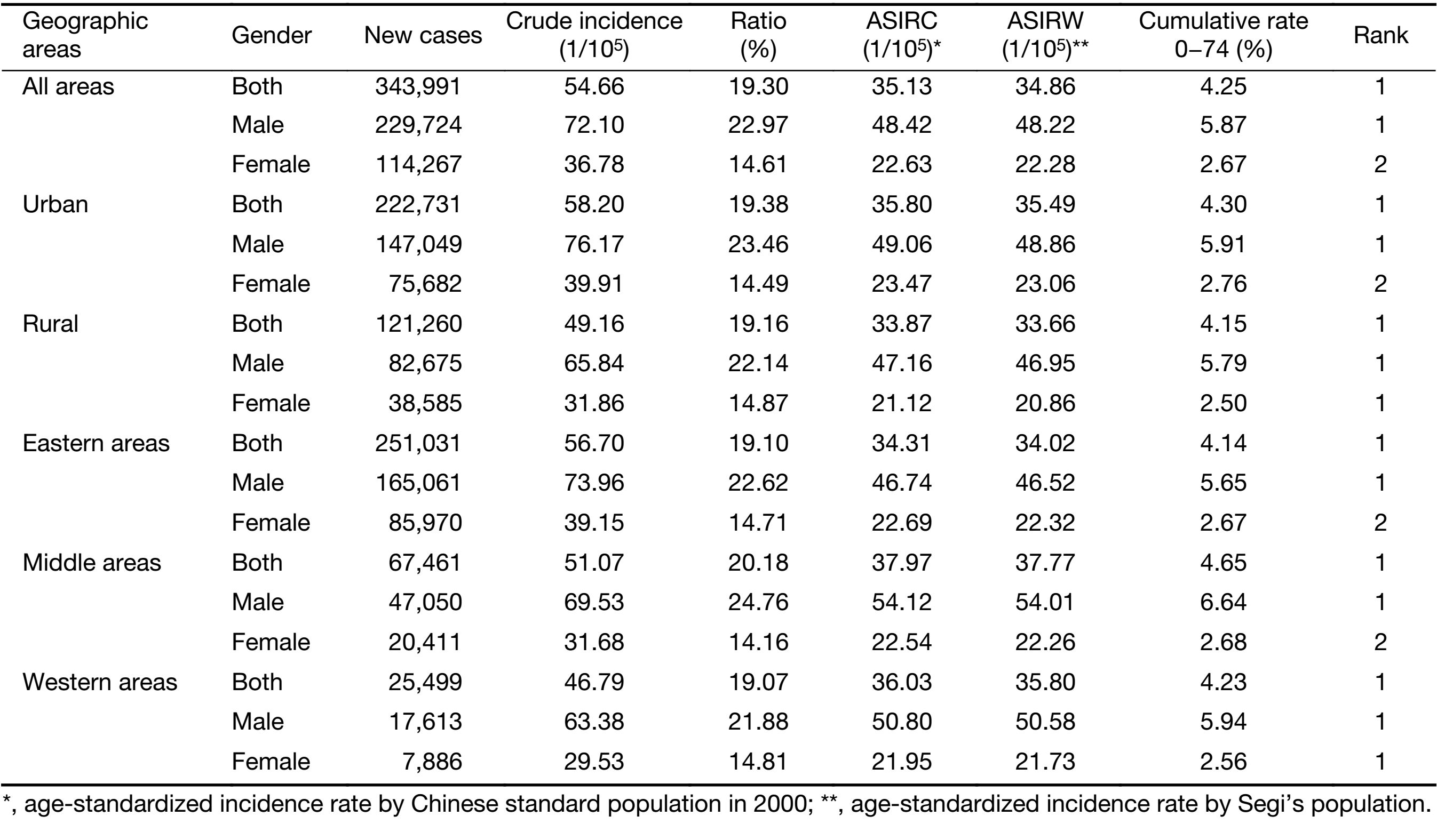
The new cases diagnosed with lung cancer of China from 2008 to 2012 was 343,991 (229,724 for males and 114,267 for females), accounting for 19.30% of all new cancer cases. The crude incidence rate of lung cancer was 54.66/100,000 which was the most common cancer in all cancer sites. The age-standardized incidence rates by China population (ASIRC) and by World population (ASIRW) were 35.13/100,000 and 34.86/100,000, respectively. The cumulative incidence rate of lung cancer before 75 years old was 4.25%. For males, lung cancer was the most common cancer, with a crude incidence of 72.10/100,000, ASIRC of 48.42/100,000 and ASIRW of 48.22/100,000. For females, lung cancer was the second most common cancer, with a crude incidence of 36.78/100,000, ASIRC of 22.63/100,000 and ASIRW of 22.28/100,000.
The incidence in urban areas was higher than that in rural areas. The crude incidence rate, ASIRC and ASIRW of lung cancer were 58.20/100,000, 35.80/100,000 and 35.49/100,000 in urban areas, with a cumulative rate of 4.30% (0−74 years old), and 49.16/100,000, 33.87/100,000 and 33.66/100,000 in rural areas, with a cumulative rate of 4.15% (0−74 years old).
The crude incidence in eastern areas was the highest (56.70/100,000) compared with middle areas (51.07/100,000) and western areas (46.79/100,000). However, ASIRC and ASIRW in middle areas were the highest (37.97/100,000, 37.77/100,000), followed by western areas (36.03/100,000, 35.80/100,000) and eastern areas (34.31/100,000, 34.02/100,000) (Table 2).
Full table
Age-specific incidence of lung cancer
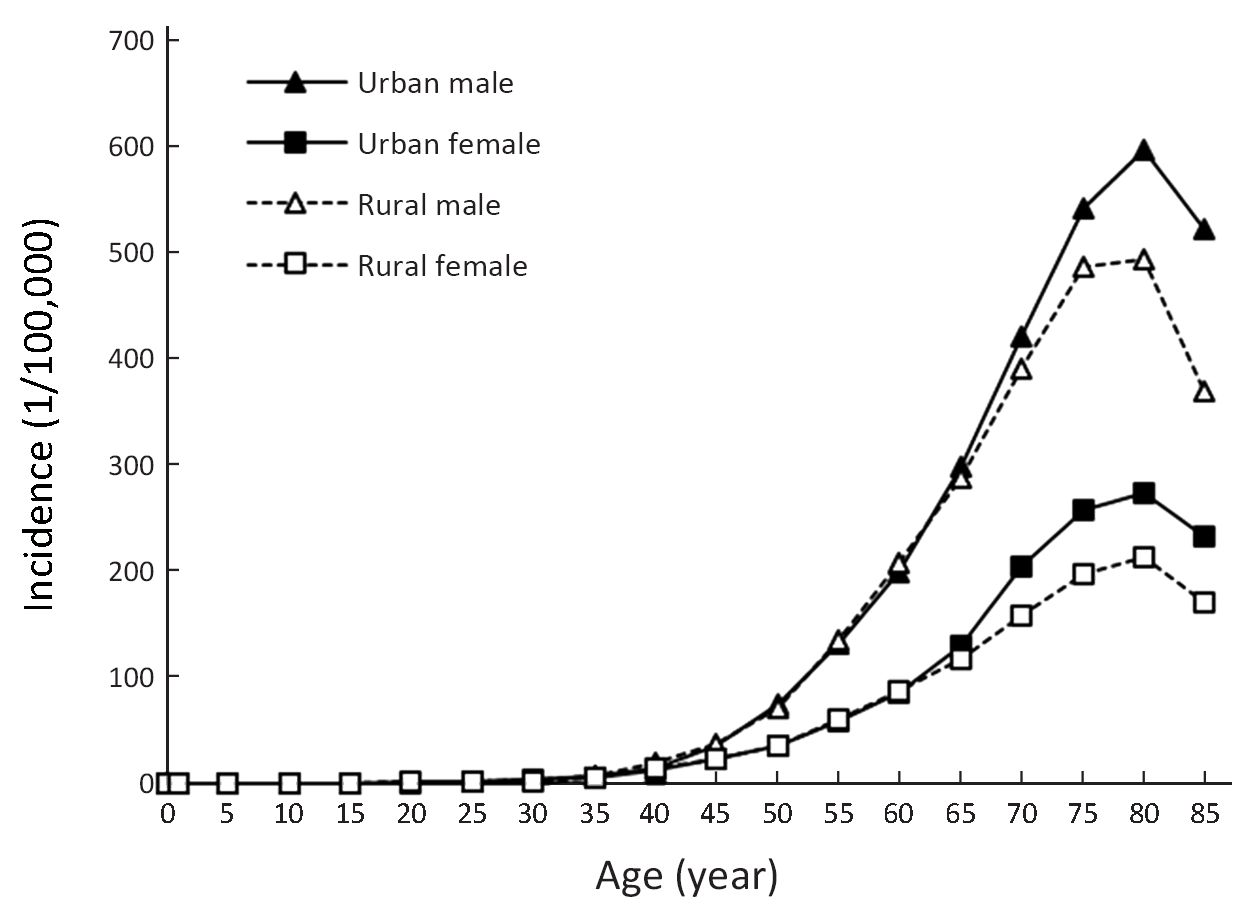
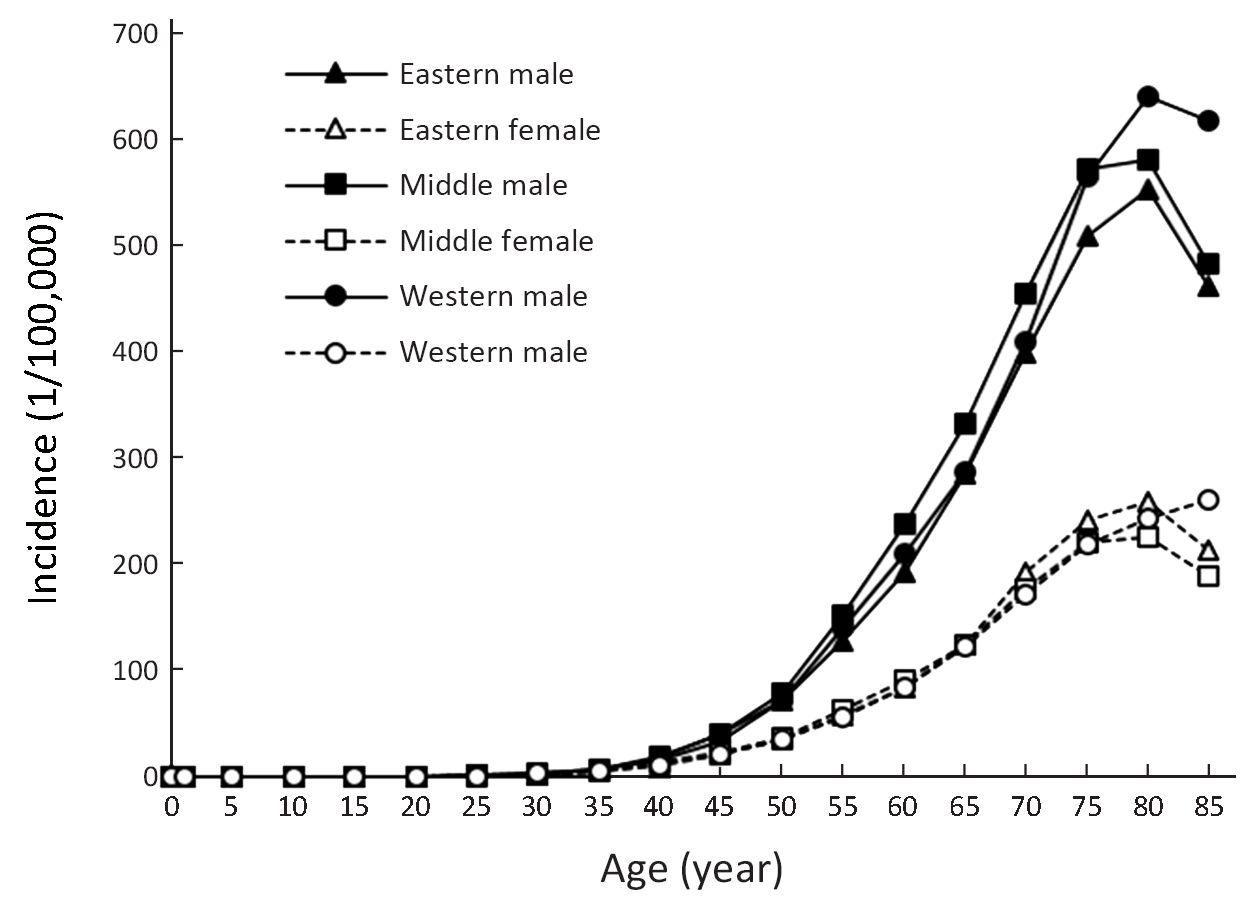
The age-specific incidence rate of lung cancer was relatively low in age groups before 40 years old and then increased with age. Among patients aged >45 years, the incidence rates were substantially higher in males than in females. The incidence rates were higher in urban areas than in rural areas among patients aged >65 years. In the age groups of 40−79 years, in males, the incidence rate in middle areas was higher than that in eastern areas and western areas, while in females, the incidence rates of the three regions were basically the same. In all regions, the age-specific incidence of males and females in the 80−84 age group was the highest (Figure 1, 2).
Temporal trend of lung cancer incidence
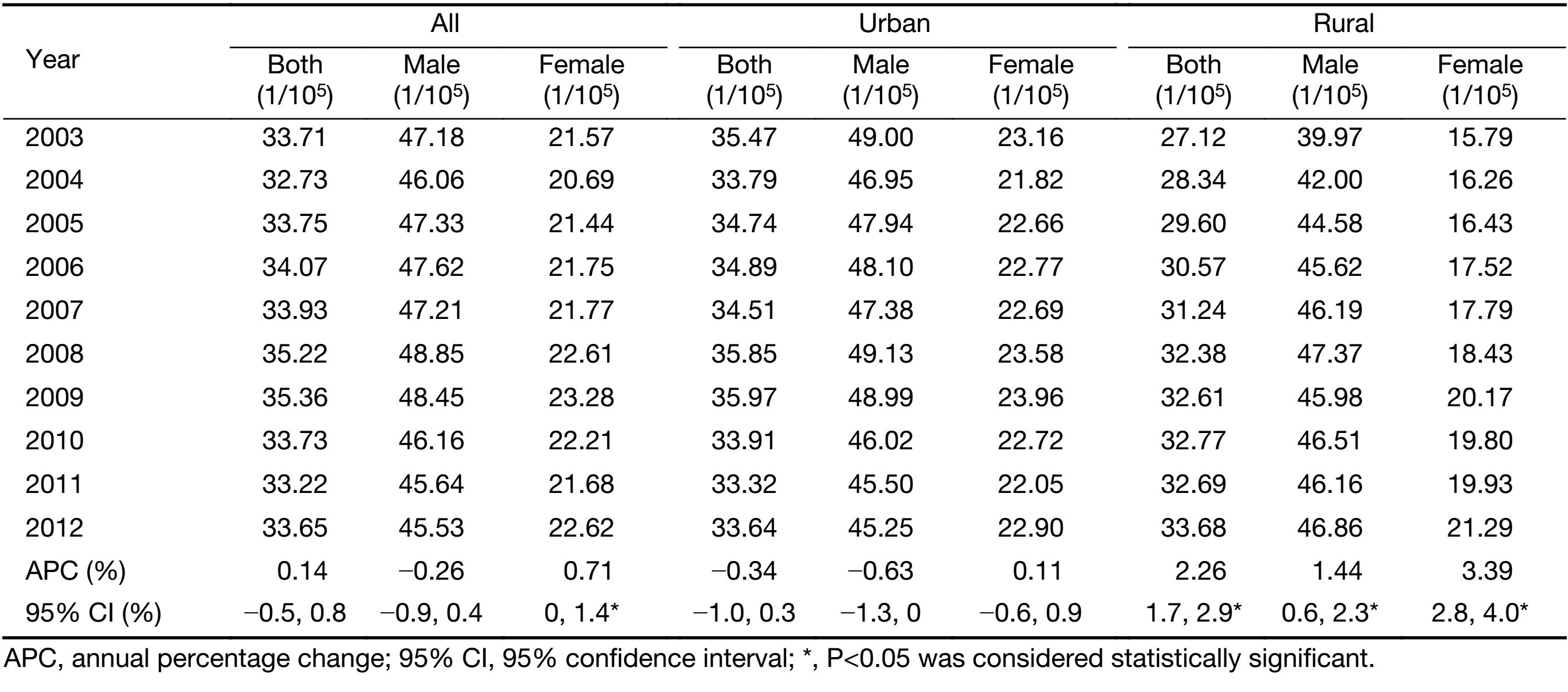
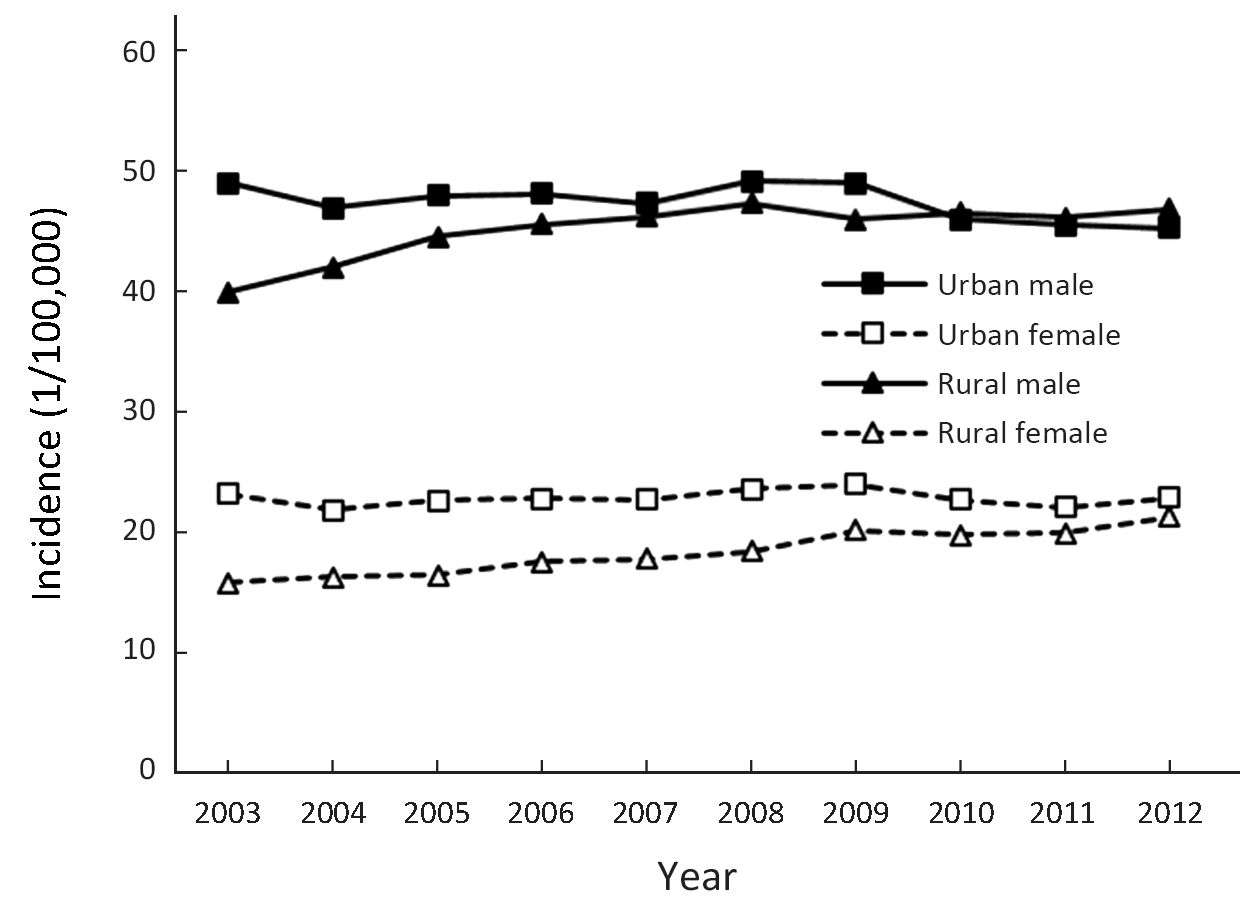
Over the past decades during 2003−2012, the temporal trend of the incidence rate of lung cancer in both sexes in China was general stable [APC: 0.14%; 95% confidence interval (95% CI): −0.5%, 0.8%]. Only in females, the lung cancer incidence rate increased by 0.71% per year, which was attributed to the rise in lung cancer incidence rates among rural females. In urban areas, the temporal trend of the incidence rate was slightly declined without statistical significance. In rural areas, the incidence rate of lung cancer increased by 2.26% per year, and in males the rate increased by 1.44% per year and in females the APC was 3.39% (95% CI: 2.8%, 4.0%) (Table 3, Figure 3).
Full table
Mortality rate of lung cancer
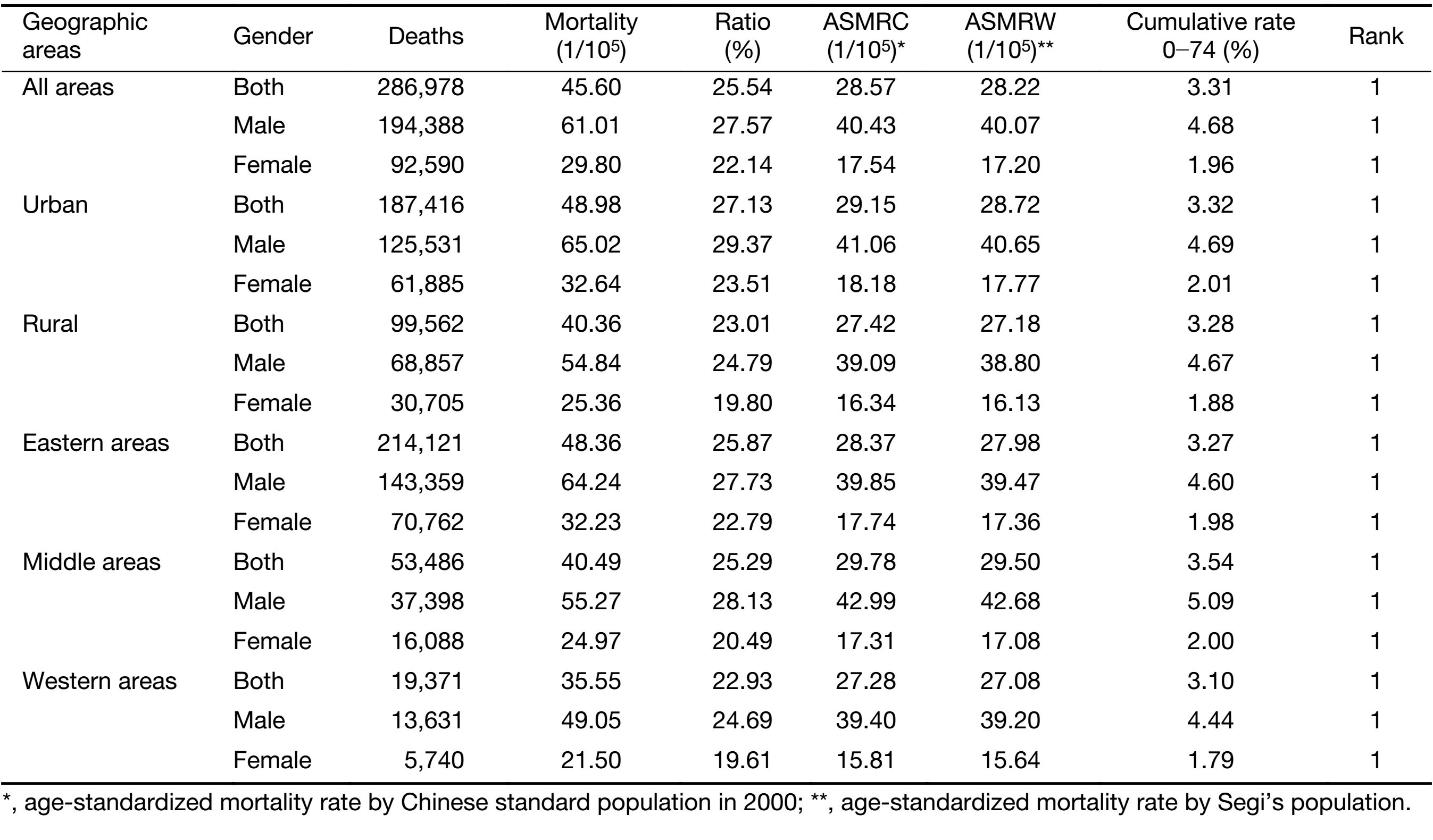
During 2008−2012, there were 286,978 patients (194,388 for males and 92,590 for females) died from lung cancer in China, accounted for 25.54% of all cancer deaths. The lung cancer crude mortality rate was 45.60/100,000, which was the leading cause of cancer-related death. The age-standardized mortality rates by Chinese standard population (ASMRC) and by world standard population (ASMRW) were 28.57/100,000 and 28.22/100,000 respectively. The cumulative mortality rate (0−74 years) was 3.31%.
Lung cancer was the first leading cause of cancer death in both urban and rural areas (4). The mortality rates were higher in males than in females (crude mortality: 61.01/100,000 vs. 29.80/100,000; ASMRC: 40.43/100,000 vs. 17.54/100,000 and ASMRW: 40.07/100,000 vs. 17.20/100,000). The mortality rates in urban areas were higher than that in rural areas (crude mortality: 48.98/100,000 vs. 40.36/100,000; ASMRC: 29.15/100,000 vs. 27.42/100,000, ASMRW: 28.72/100,000 vs. 27.18/100,000) (Table 4).
Full table
The eastern areas had a high crude mortality rate (48.36/100,000), followed by the middle (40.49/100,000) and western areas (35.55/100,000). After adjusted by age, the middle areas had the highest mortality rate (ASMRC: 29.78/100,000; ASMRW: 29.50/100,000) and the mortality in eastern areas (ASMRC: 28.37/100,000; ASMRW: 27.98/100,000) was higher than that in western areas (ASMRC: 27.28/100,000; ASMRW: 27.08/100,000) (Table 4).
Age-specific mortality rate of lung cancer
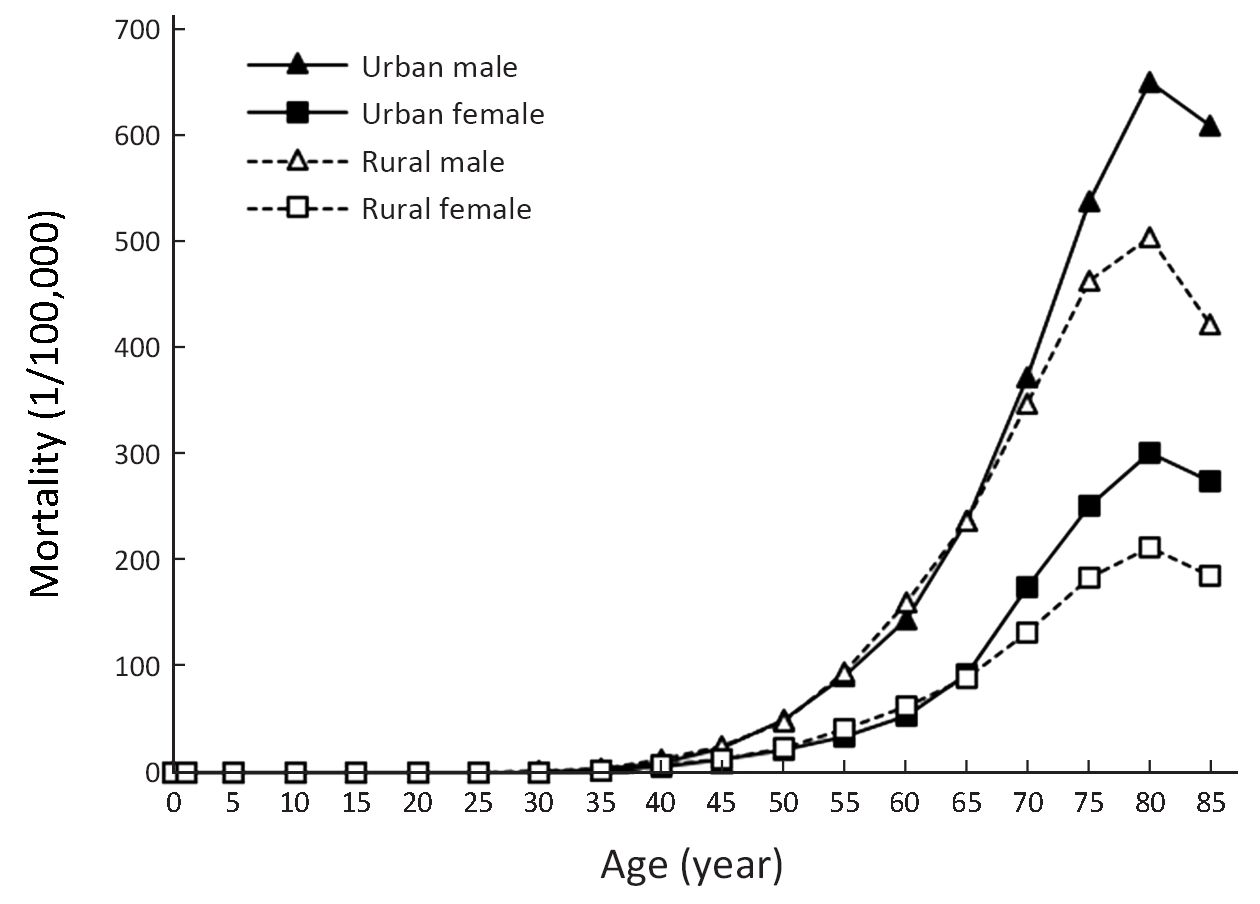
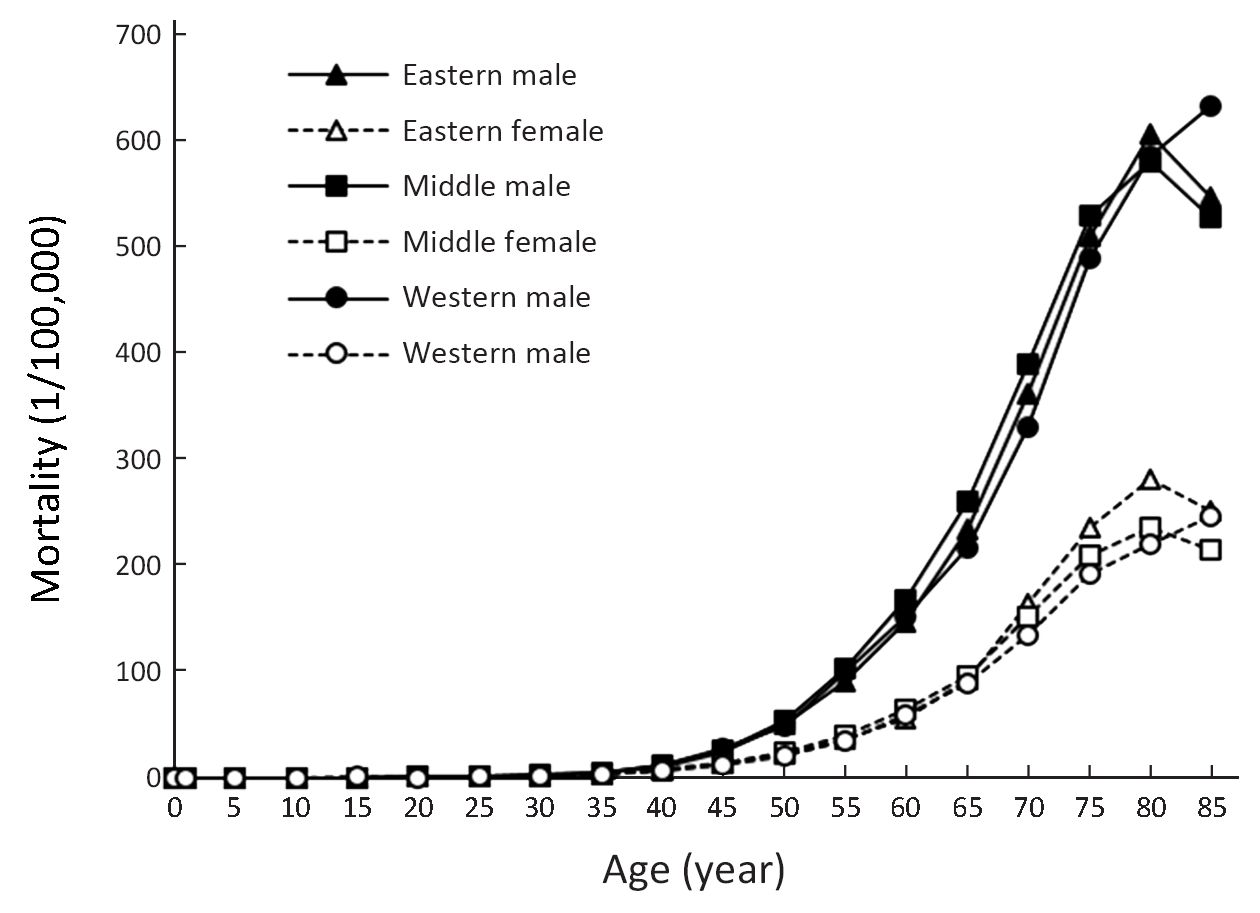
Because of a high mortality rate, the patterns of age-specific mortality rates of lung cancer were close to those of age-specific incidence rates. Among patients aged >45 years, mortality rates among males were significantly higher than those among females. There was a higher mortality rate in urban areas than in rural areas for males and females in groups aged over 70 years old. The mortality rate of lung cancer was similar in eastern areas, middle areas and western areas for males and females. The mortality rate peaked in the 80−84 age groups in urban and rural areas. In eastern areas, middle areas and western areas, the mortality rate peaked in the 80−84, 80−84 and 85+ age groups, respectively (Figure 4, 5).
Temporal trend of lung cancer mortality
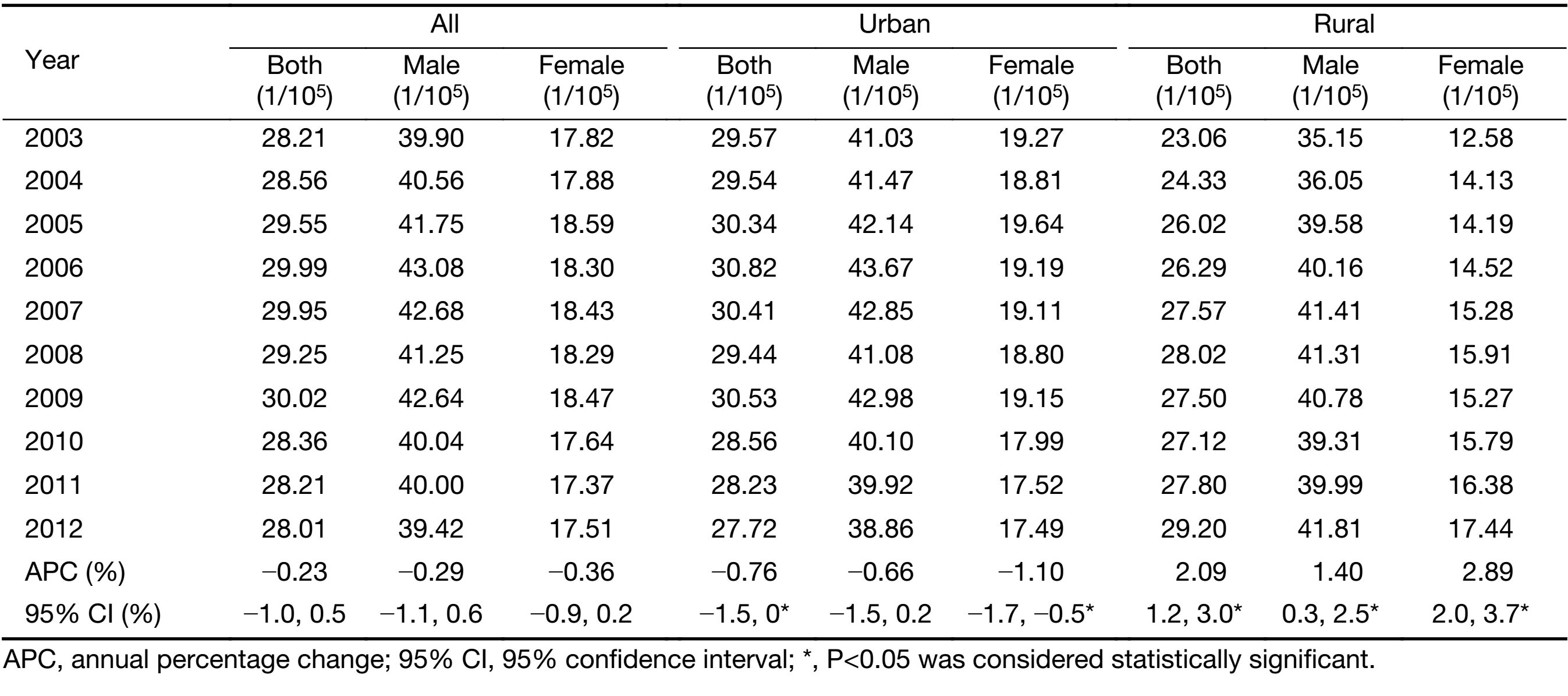
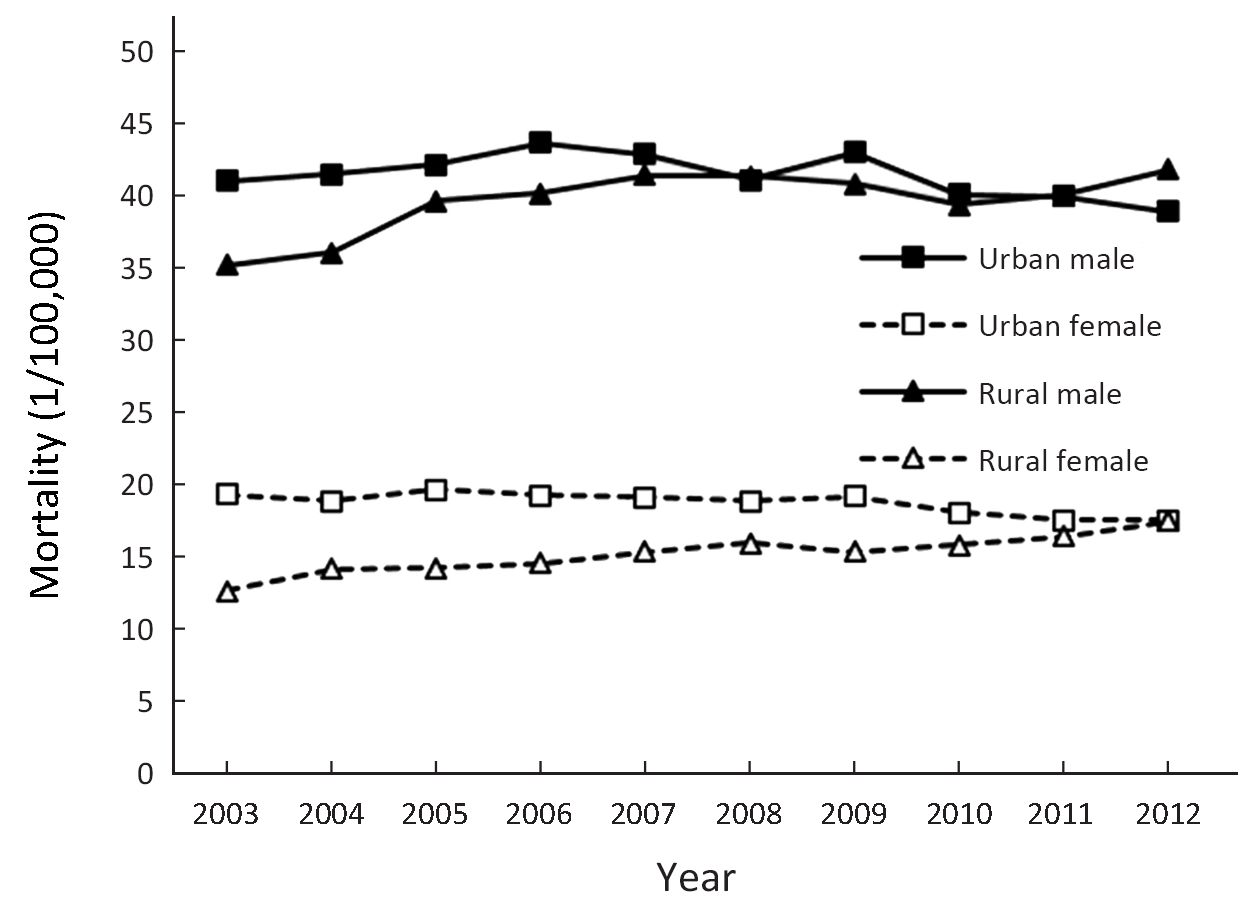
The mortality rate of lung cancer decreased slightly annually over the decades from 2003 to 2012 in China (APC: −0.23%; 95% CI: −1.0%, 0.5%; P>0.05). In males the mortality rate reduced by 0.29% per year (P>0.05) and in females the APC of the rate was −0.36% (95% CI: −0.9%, 0.2%). Over the past decade, mortality rates of lung cancer are two distinct temporal trends in urban and rural areas in China. In urban areas, the mortality rate of lung cancer declined by 0.76% per year in both sexes (P<0.05), and reduced by 1.10% per year in females (P<0.05). In contrast to the declining trends in the urban areas, the mortality rates of lung cancer in rural areas during 2003−2012 rose by 1.40% in males and by 2.89% in females per year (Table 5, Figure 6).
Full table
Discussion
Lung cancer is the most frequent malignant neoplasm in most countries, and the main cancer-related cause of mortality worldwide in both sexes combined (1). In China, there were an estimated 343,991 new cases of lung cancer (19.30% of total cancer incidence cases) and 286,978 lung cancer-related deaths (25.54% of total cancer mortality cases) during 2008−2012, which made lung cancer ranked first in the cancers for both incidence and mortality.
Many risk factors have been identified for lung cancer. The tobacco consumption is the main etiological factor in lung carcinogenesis (7). And the incidence and mortality of lung cancer are chiefly determined by tobacco consumption on a population level. Other risk factors, such as genetic susceptibility, poor diet, occupational exposures and air pollution, may act independently or in concert with smoking in shaping the descriptive epidemiology of lung cancer (8).
The incidence of lung cancer was higher in males than in females in China. The ratio of male to female was 1.96:1 in China, 1.91:1 in urban areas and 2.07:1 in rural areas. The reasons for higher incidence in males probably reflect the different smoking rate between males and females: 57.4% of males and 2.6% of females smoke in China in 2002 (9). Duration of smoking should be considered the strongest determinant of lung cancer risks in smokers (10). However, passive smoking and indoor environment of cooking smoke were probably the main risks of lung cancer for non-smoking women (11). Although more natural gas is now used as fuel in urban areas, coal, biomass, and other fuels remain the main energy sources in vast rural areas.
The incidence of lung cancer was higher in more developed regions than in less developed regions worldwide, predominantly related to smoking habits, but overall incidence is decreasing in developed countries due to tobacco control policies (12,13). Our study showed that there was higher incidence of lung cancer in urban areas than in rural areas. The geographic and temporal patterns of the disease largely reflect tobacco consumption accumulated during previous decades (14). In China, cigarette consumption became widespread earlier in urban areas than in rural areas, mainly because of limited rural availability and affordability of cigarettes (15). However, this urban versus rural difference is likely to diminish, or even be reversed, because rural men born after the 1960s not only tended to start at the same age as urban men and to smoke only cigarettes, but also had a somewhat higher smoking prevalence (15). In 2002, the smoking rate in urban areas was already lower than that of rural areas (29.5% vs. 37.8%) in China (9). In accordance with this, the reduced rate ratio of urban areas to rural areas from 2.07 to 1.14 during 1989−2008 in China was reported (16). In our study, there was statistically great increment of incidence and mortality of lung cancer in rural areas in China during 2003−2012, especially for females.
Conclusions
Lung cancer is the most common cancer in China and showed an increasing trend of rate in rural areas in recent years, especially for females. There are disparities of incidence rate in genders, age groups and different areas. Appropriate targeted prevention, early detection and treatment programs can be carried out to control the local burden of lung cancer.
Acknowledgements
We thank the Bureau of Disease Control, National Health and Family Planning Commission of the People’s Republic of China for their support to this study. We gratefully acknowledge all the population-based cancer registries for the effort they put in data collection, data sorting, data verification and database creation. The authors take full responsibility for analyses and interpretation of these cancer registry data.
Footnote
Conflicts of Interest: The authors have no conflicts of interest to declare.
References
- Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018;68:394–424. [PubMed] DOI:10.3322/caac.21492
- Zheng R, Zeng H, Zuo T, et al. Lung cancer incidence and mortality in China, 2011. Thorac Cancer 2016;7:94–9. [PubMed] DOI:10.1111/1759-7714.12286
- Chen W, Zheng R, Zuo T, et al. National cancer incidence and mortality in China, 2012. Chin J Cancer Res 2016;28:1–11. DOI:10.3978/j.issn.1000-9604.2016.02.08
- Chen W, Zheng R, Zhang S, et al. Cancer incidence and mortality in China in 2013: an analysis based on urbanization level. Chin J Cancer Res 2017;29:1–10. [PubMed] DOI:10.21147/j.issn.1000-9604.2017.01.01
- National Cancer Center. Chinese Guideline for Cancer Registration. Beijing: People’s Medical Publishing House, 2016.
- Curade MP, Edwards B, Shin HR, et al. Cancer incidence in five continents. Volume IX. IARC Sci Publ 2008:1-837.
- de Groot PM, Wu CC, Carter BW, et al. The epidemiology of lung cancer. Transl Lung Cancer Res 2018;7:220–33. [PubMed] DOI:10.21037/tlcr.2018.05.06
- Malhotra J, Malvezzi M, Negri E, et al. Risk factors for lung cancer worldwide. Eur Respir J 2016;48:889–902. [PubMed] DOI:10.1183/13993003.00359-2016
- Yang GH, Ma JM, Liu N, et al. Smoking and passive smoking in Chinese, 2002. Zhonghua Liu Xing Bing Xue Za Zhi (in Chinese) 2005;26:77–83. [PubMed] DOI:10.3760/j.issn:0254-6450.2005.02.001
- Doll R, Peto R, Boreham J, et al. Mortality in relation to smoking: 50 years’ observations on male British doctors. BMJ 2004;328:1519. [PubMed] DOI:10.1136/bmj.38142.554479.AE
- Zhang X, Wu L, Xu Y, et al. Trends in the incidence rate of lung cancer by histological type and gender in Sichuan, China, 1995-2015: A single-center retrospective study. Thorac Cancer 2018;9:532–41. [PubMed] DOI:10.1111/1759-7714.12601
- Torre LA, Siegel RL, Jemal A. Lung Cancer Statistics. Adv Exp Med Biol 2016;893:1–19. [PubMed] DOI:10.1007/978-3-319-24223-1_1
- Youlden DR, Cramb SM, Baade PD. The International Epidemiology of Lung Cancer: geographical distribution and secular trends. J Thorac Oncol 2008;3:819–31. [PubMed] DOI:10.1097/JTO.0b013e31818020eb
- Peto R, Lopez AD, Boreham J, et al. Mortality from tobacco in developed countries: indirect estimation from national vital statistics. Lancet 1992;339:1268–78. [PubMed] DOI:10.1016/0140-6736(92)91600-D
- Chen Z, Peto R, Zhou M, et al. Contrasting male and female trends in tobacco-attributed mortality in China: evidence from successive nationwide prospective cohort studies. Lancet 2015;386:1447–56. [PubMed] DOI:10.1016/S0140-6736(15)00340-2
- Zou X, Jia M, Wang X, et al. Changing epidemic of lung cancer & tobacco and situation of tobacco control in China. Zhongguo Fei Ai Za Zhi (in Chinese) 2017;20:505–10. [PubMed] DOI:10.3779/j.issn.1009-3419.2017.08.01