
Annual report on status of cancer in China, 2010
Introduction
Population-based cancer registry collects the data on cancer incident cases and deaths from covered population to describe and surveillance the cancer epidemics in certain areas. The cancer registration data are not only applied for cancer control planning, implementation and evaluation on cancer prevention and control but also for scientific research (1). Since 2006, when Disease Prevention and Control Bureau, Health and Family Planning Commission of China started to publish cancer statistics annually, National Central Cancer Registry (NCCR) of China has been responsible for collecting data from all local registries, calculating the statistical items accurately, and analyzing the data of cancer incident cases and deaths from registration areas, then released the updated data in Cancer Registry Annual Report (2). The cancer statistic data have been broadly utilized in scientific researches, clinical trials and decision of cancer prevention and control strategies.
Materials and methods
Data source
The NCCR collected cancer registration data from population-based cancer registries in China. Total 219 registries submitted cancer registration data in 2010 to NCCR. They were distributed in 28 provinces, autonomous regions or municipalities. The registries identified new cancer cases from all hospitals, community health centres, medical insurance and death registries (for cases only identified by death certification). Registries obtained information on cancer deaths from the death surveillance system, which collects death information from hospitals and the Civil Administration Bureau with available cremation records. Population information was collected from local statistic bureau or household register department in local public security bureau.
Quality control
Submitted data were checked and evaluated by NCCR based on “Guideline for Chinese Cancer Registration” and referring to relevant data quality criterion of “Cancer Incidence in Five Continents Volume IX” by International Agency for Research on Cancer/International Association of Cancer Registries (IARC/IACR) (3). Proportion of MV%, percentage of cancer cases identified with DCO%, M/I, percentage of uncertified cancer (UB%) and percentage of cancer with undefined or unknown primary site (secondary) (O&U%) were used to evaluate the completeness, validity and reliability of cancer statistics.
Statistical analysis
Cancer incident cases and deaths were stratified by areas (urban/rural), region (eastern, middle, western), cancer type, sex (male, female), and age (grouped by 0, 1-4, 5-9, …, 80-84, 85 years old and above). Age-specific rate was used for estimates of incidence and death in 2010. Crude incidence rate, mortality, proportion and cumulative rate were calculated using the national population in 2010. The 2000 Chinese census population and world Segi’s population were applied for the calculation of age-standardized rates. Database software, including MS-FoxPro, MS-Excel, SAS and IARCcrgTools issued by IARC/IACR (4), were used for data check, evaluation and calculation.
Results
Data quality
There were 145 registries accepted by this annual report distributed in 28 provinces, including 63 cities and 82 counties covered 158,403,248 of populations, including 80,355,188 males and 78,048,060 females, accounted for 11.86% of whole national population in 2010.
The overall indicators of MV%, DCO%, and M/I ratio were 67.11%, 2.99% and 0.61, respectively. They were 71.51%, 2.49% and 0.59 in urban registries, compared to 60.65%, 3.72% and 0.64 in rural. The quality evaluation for major cancers is presented in Table 1.

Full table
Incidence and mortality of overall cancers
Incidence
It was estimated there were 3,093,039 new cases diagnosed as cancer in 2010. The crude incidence rate of all cancers was 235.23/100,000 (268.65/100,000 in males and 200.21/100,000 in females). The age-standardized incidence rates were 184.58/100,000 and 181.49/100,000 by Chinese population (ASIRC) and World population (ASIRW), respectively. Among the patients aged 0-74 years, the cumulative incidence rate was 21.11%. The crude cancer incidence rate and age-standardized rates in urban areas were higher than that of rural areas. The crude incidences in males and females were higher in urban than that in rural. However, after adjusted by age, cancer incidences for men in urban and rural were conversed. More new cancer cases occurred in eastern areas than middle areas and western areas, however, crude incidence rates in three areas were not greatly different (Table 2).

Full table
Age-specific incidence rate
Cancer incidence was relatively lower before 39 years old, then increased dramatically after 40 years old, and finally peaked after 80 years and then slightly decreased after 85 years (Table 3, Figure 1). The pattern was similar between urban and rural areas. Comparing the age-specific incidence rate between urban and rural areas, except age from 55-64 years, urban had higher incidence rates in most of age groups. Group of 80 years was higher in urban areas than in rural areas, but lower in the age-group of 40-74 years. Before age of 70 years, most age groups of males in rural had higher incidence rate than that in urban. However, in females, the incidences were higher in urban than that in rural areas in every age group after 25 years (Table 3, Figure 1).


Full table
Mortality
It was estimated there were 1,956,622 died from cancer in 2010. The crude mortality of all cancers in China was 148.81/100,000 (186.37/100,000 in males and 109.42/100,000 in females). The age-standardized mortalities were 113.92/100,000 and 112.86/100,000 by Chinese population (ASMRC) and World population (ASMRW), respectively. Among the patients aged 0-74 years, the cumulative incidence rate was 12.78%. The crude cancer incidence rate and age-standardized rates in urban areas were higher than that in rural areas. The crude cancer mortalities were higher in urban than in rural. However, after adjusted by age, mortalities were conversed both in males and females. More cancer deaths occurred in eastern areas than middle areas and western areas, however, western areas had higher mortalities than eastern and middle areas (Table 4).

Full table
Age-specific mortality
The cancer mortality was relatively lower before 50 years and then dramatically increased reaching peak after 85 years (Table 5, Figure 2). The mortality in rural areas was highest in the age-group of 80-84 years. The age-specific mortality in urban men was lower than that in rural in most of age-groups before 80 years old. In female, the mortality in urban was higher than that in rural only for age group over 75 years.

Full table

Incidence and mortality for major cancers
Cancer incidence of the ten most common cancers
Lung cancer was the most common cancer in all areas, followed by female breast cancer, stomach cancer, liver cancer and esophageal cancer with estimated new cases of 605,946, 208,192, 404,565, 358,840, and 287,632, respectively. Lung cancer was the most frequently diagnosed cancer in males followed by stomach cancer, liver cancer, esophageal cancer and colorectal cancer. Breast cancer was the most common cancers in females followed by lung cancer, colorectal cancer, stomach cancer and liver cancer (Table 6).

Full table
Cancer death of the ten most common cancers
Lung cancer was the leading cause of death in China followed by liver cancer, stomach cancer, esophageal cancer and colorectal cancer with estimated deaths of 486,555, 312,432, 287,851, 208,473, and 132,110, respectively. In males, lung cancer was the leading cause followed by liver cancer, stomach cancer, esophageal cancer and colorectal cancer; while in females, lung cancer was still the leading cause followed by stomach cancer, liver cancer, esophageal cancer and breast cancer (Table 7).

Full table
Cancer incidence of the ten most common cancers in urban areas
In urban areas, lung cancer was the most frequently diagnosed cancer, followed by female breast cancer, stomach cancer, colorectal cancer and liver cancer with the estimated new cases of 348,107, 127,707, 193,832, 176,942, and 166,166, respectively. The most common sites of cancer were lung, stomach, liver, colon-rectum and esophagus in males, while were breast, lung, colon-rectum, stomach and liver in females (Table 8).

Full table
Cancer death of the top ten most common cancers in urban areas
Lung cancer was the leading cause of cancer death in urban areas for both men and women with number of deaths and mortalities of 192,438, 56.72/100,000, 87,481, 27.04/100,000, respectively. Other cancer types with high mortality in men were liver cancer, stomach cancer, esophageal cancer and colorectal cancer. In women, stomach cancer was the second cause of cancer death, followed by liver cancer, colorectal cancer and breast cancer (Table 9).

Full table
Cancer incidence of the ten most common cancers in rural areas
Table 10 shows the ten most common cancer incidence rates in rural areas. Lung cancer had been becoming the most frequently diagnosed cancer (257,839 new cases with incidence rate of 39.54/100,000), followed by stomach cancer, liver cancer, esophagus cancer and female breast cancer. The most common sites of cancer in men were lung, stomach, liver, esophagus and colon-rectum, while in women, were breast, lung, stomach, esophagus and liver.

Full table
Cancer death of the top ten most common cancers in rural areas
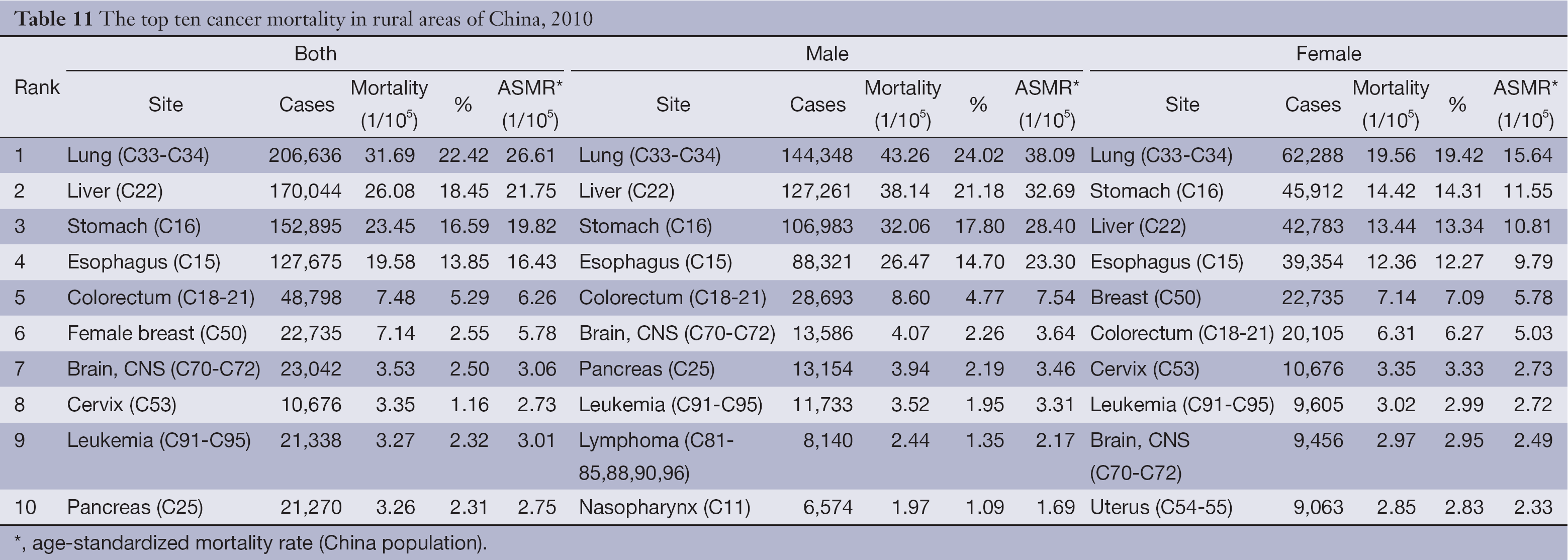
Lung cancer was the leading cause of cancer death in rural areas for both men and women. The number of deaths on lung cancer in rural was 206,636 with mortality of 31.69/100,000. The other cancer types with high mortality were liver cancer, stomach cancer, esophageal cancer and colorectal cancer in male; stomach cancer, liver cancer, esophageal cancer and breast cancer in female (Table 11).
Full table
Discussion
In 2010, the program registries covered by the National Program of Cancer Registry were 193. When NCCR called for data submission, total 219 registries reported registration data including voluntary registries. The population coverage of these registries was over 200 millions, accounted for 15% of national populations. A couple of registries are established every year under financial support from national program. In 2013, the number of registries has been increased to about 250. IARC/IACR recently released the new version of “Cancer Incidence in Five Continents, Volume X” (http://ci5.iarc.fr/CI5-X/ci5-X.htm). There were 12 registries from mainland China accepted for the publication.
In order to ensure the quality of registration data, NCCR processes the data based on the national criteria issued in program protocol. The incidence, mortality and population have to keep reasonable levels compared to past data and similar areas. If unexplicable, data would be sent back to registries to check. The indicators of completeness, comparability and invalidity, such as, MV%, DCO%, M/I ratio, UB% and O&U% were evaluated for each registry’s data to judge if submitted data are valid or not. Through the double evaluations in provincial and national level, 154 registries were qualified and accepted for final database. The valid data were pooled and analyzed for cancer statistics in 2010. This is the first time that cancer incident new cases and cancer deaths were estimated based on the available data making results more practical.
The results showed the estimated cancer incident cases were 3.09 millions and 1.96 cancer deaths in 2010 with the incidence rate of 235.23/100,000 and mortality of 148.81/100,000. Compared to the figures in 2009, both incidence and mortality were slightly lower (5). The reason of the decrease might be the dramatic increase of coverage of population. However, the cancer spectrum was as same as that in the previous year. In this study, the data were stratified by areas (eastern, middle, and western) and it was found that the incidence and mortality were not quite different for overall cancers. Although the number of registries has been double than in 2009, coverage in western areas was still so limited and the representativeness was needed to be evaluated (6).
Urban China had a higher cancer incidence and lower mortality than rural and the cancer patterns are quite different (7,8). It hints different cancer control strategies should be implemented according to different cancer statistics. Lung cancer becomes the most common cancer and the leading cancer death both in urban and rural areas, and especially, in rural, it has replaced liver cancer or stomach cancer as the first killer before. Recently, IARC published an updated issue about air pollution and cancer to firstly identify air pollution is strongly associated with cancer. It was estimated that more than half of the lung cancer deaths are attributable to ambient fine particles in China (http://www.iarc.fr/en/publications/books/sp161/index.php). However, the etiology of lung cancer in rural should be emphasized. Same as lung cancer, breast cancer has become the most common cancer in women in rural areas. The changes of lifestyle, diet and environment have impacted on both urban and rural women.
China is facing critical health issues caused by cancer with over 3 million new cases and nearly 2 million cancer deaths annually. Risk factors, such as air pollution, infection, and changes of diet habit and lifestyle, maintain high level in Chinese, so that, the cancer burden is getting serious. Cancer control strategies, including health education, health promotion, early detection and cancer screening, should be treated as priority in public health. As the fundamental work, cancer registration plays an important role on cancer control and should be emphasized.
Acknowledgements
We gratefully acknowledged the cooperation of all the population-based cancer registries in providing cancer statistics, data collection, sorting, verification and database creation. The authors assume full responsibility for analyses and interpretation of these data.
Disclosure: The authors declare no conflict of interest.
References
- Parkin DM. The evolution of the population-based cancer registry. Nat Rev Cancer 2006;6:603-12. [PubMed]
- National Office for Cancer Prevention and Control, National Center for Cancer Registry, Disease Prevnetion and Control Bureau, MOH. Chinese Cancer Registry Annual Report (2012). Beijing: Military Medical Science Press, 2012:12.
- Curado MP, Edwards B, Shin HR, et al. Cancer Incidence in Five Continents. Vol. IX. IARC Scientific Publications No.160. Lyon: IARC, 2008:1-837.
- Ferlay J. The IARC crgTools Programs. Avaiable online: http://wwwiacrcomfr/iarccrgtooshtmIACR 2006
- National Office for Cancer Prevention and Control, National Center for Cancer Registry, Disease Prevnetion and Control Bureau, MOH. Chinese Cancer Registry Annual Report (2011). Beijing: Military Medical Science Press, 2011:12.
- Li GL, Chen WQ. Representativeness of population-based cancer registration in China--comparison of urban and rural areas. Asian Pac J Cancer Prev 2009;10:559-64. [PubMed]
- Chen WQ, Zheng RS, Zeng HM, et al. Trend analysis and projection of cancer incidence in China between 1989 and 2008. Zhonghua Zhong Liu Za Zhi 2012;34:517-24. [PubMed]
- Zeng HM, Zheng RS, Zhang SW, et al. Trend analysis of cancer mortality in China between 1989 and 2008. Zhonghua Zhong Liu Za Zhi 2012;34:525-31. [PubMed]